Juniper Publishers : Clinical Study: Effect of Supplementation with High Genistein Soybean Isoflavones and Pumpkin Standardized Extract on Urinary Incontinence in Western Perimenopausal Women
JUNIPER PUBLISHERS- JOURNAL OF GYNECOLOGY AND WOMEN’S
HEALTH

Journal of Gynecology and Women’s Health-Juniper
Publishers
Authored by Marañón JA*
Abstract
Objective: To examine the effect of
supplementation of a novel combination of high genistein soybean extract
and pyrogallol plus polyphenols from standardized pumpkin seed extract
in perimenopausal women with urinary (UI) incontinence.
Methods: The present study investigated the
effects of a dietary supplement formula containing high genistein
soybean extract and pumpkin seed extract (DROPSORDRY™) on 82
perimenopausal women diagnosed with urinary incontinence. Subjects
received 2 tablets of DROPSORDRY™ per day for 4 weeks, followed by 1
tablet per day for an additional 4 weeks. Subjects recorded UI symptoms
and quality of life before supplementation for 14 days and for 8 weeks
during treatment. Paired difference test (Wilcoxon test) was used to
determine if there was a significant improvement in UI symptoms before
and after treatment.
Results: Compared to baseline data,
statistically significant decreases were observedin mean urgency grade
(24.7%; P<0.01), nocturia (69.35%; P<0.05) and the use of daily
pantyliners (66.25%; p<0.01). In addition, in the quality of life was
improved in 92.3% of the subjects.
Conclusion: The results suggest that
DROPSORDRY™ supplementation is a safe and an effective strategy for
reducing urinary incontinence symptoms and quality of life in Western
perimenopause women.
Keywords: Dietary
supplements; Urinary incontinence; Perimenopause; Genistein; Pyrogallol;
Soybean extract; Pumpkin seed extract; Stress urinary incontinence
(SUI) Introduction
Urinary incontinence (UI) is a significant health
problem with considerable social and economic impact. According to the
National Association for Continence, UI affects over 25 million people
in the U.S., of which 75-80% are women [1].
UI affects women of all ages, and risk factors include pregnancy,
childbirth, body mass index, previous hysterectomy and menopause [2]. The prevalence of UI also increases with age [3].
UI is divided into three major subtypes. Stress
urinary incontinence (SUI) is defined as involuntary loss of urine
resulting from physical exertion, or from sneezing or coughing.Urgency
urinary incontinence (UUI) is involuntary leakage accompanied by the
sudden need to pass urine. UUI will also manifest as frequency and
nocturia (frequent urination at night). Mixed urinary incontinence is a
combination of both [4,5].
When UI is combined with frequency and urge (or both), it is described
as Overactive bladder syndrome (OAB). OAB affects an estimated 7.6% of
women in the U.S [6].
UI and OAB result in significant decrease in quality of life [3,4,7,8], and a number of studies have also indicated that UI results in substantial economic burden [7,9].
One analysis reported that a patient's willingness to pay for
improvement exceeds routine care costs by 3-7 times. Therefore effective
treatment may be economically beneficial as well as improving quality
of life. 7 Current treatment for UI includes pelvic floor muscle
training, surgery, and anti-muscarinic medications. Anti- muscarinic
medications block the action of acetylcholine on the muscarinic
receptors located in the epithelial lining of the bladder, thereby
reducing abnormal bladder contractions. The overall efficacy and
tolerability profile of these medications is reported to be less than
optimal, as side effects such as constipation and dry mouth are common [10].
The etiology of UI varies between subtype with SUI
caused by sphincter weakness and UUI a result of over activity of the
detrusor muscle, the smooth muscle that lines the wall of the bladder.
This over activity may be caused by inflammation, infection or loss of
neurological control of detrusor contractions via the muscarinic
receptors [10,3].
In the case of menopause and perimenopause, other physiological changes
also increase the risk of UI. The decline in estrogen occurring during
these stages is believed to play a role, as the bladder is rich in
estrogen receptors [11]. Conversely, muscarinic receptors generally increase during menopause [12].
Morphological changes in estrogen sensitive tissue, such as thinning
and atrophy of the urethral muscle and connective tissue, also affect
continence [13].
While in theory, hormonal replacement therapy (HRT) might help reverse
the estrogen decline, it has shown mixed results in treating UI
associated with menopause [11,13,14]. In fact, in studies have shown that exogenous estrogen worsens incontinence in postmenopausal women [15-17].
In addition, HRT is associated with risks of breast, endometrial and
ovarian cancers as well as dementia and cardiovascular diseases [18].
Pelvic floor muscle training is one
non-pharmaceutical treatment for UI. However, it has been shown to be
less effective in women early menopause and in the late menopausal
transition [19]. In addition, many women transitioning to menopause may not seek out treatment for UI [20].
Therefore, there is much need for safe alternative treatment for UI
associated with menopausal transition stages that does not require
treatment from a physician or compliance to exercise therapy.
Materials and Methods
Participants
Eighty-two perimenopausal women diagnosed with
urinary incontinence (42-62 years, mean 52 years) were enrolled in this
study. The presence of UI was previously diagnosed using the
International Continence Society standards (ICS). Subjects were excluded
if they had allergies to the treatment ingredients, were pregnant or
lactating, had previously diagnosed heart disease or were currently
under pharmacological treatment. Documented informed consent was
obtained from all patients prior to the study and the study was
performed in accordance with international ethical standards of Helsinki
Declaration, and the research protocol was approved by the Comission of
Bioetics, and Biosafety of Universidad de Extremadura, Merida, Spain.
Procedure and measures
This study was a single-center, not randomized open
prospective study. Daily dosage was 2 tablets per day (500 mg of active
material) from 0 to 4 week (T1). At week 4, the dosage was reduced to
500mg/day daily intake for an additional 4 weeks (T2). Subjects were
instructed to keep a micturition diary, following the International
Consultation on Incontinence Questionnaire (ICIQ), before
supplementation (T0) for 14 days, and for 8 weeks during treatment. The
subjects monitored the time and amount of urine produced during a
24-hour period, urgency score (0-4), each incident of urine leakage due
to urge or stress, and use of panty liners. The impact of symptoms of
incontinence on quality of life and outcome of treatment was also
assessed. A physician also evaluated each patient's micturition diary
every three days, recording day, night and total frequency, day, night
and total volume, episodes and grades of urgency per day, episodes on
incontinence per day (stress and urge) and volume of urine over 24 hours
and at night.
Materials
DROPSORDRY™ is a dietary supplement in tablet form
consisting of 500mg of a mixture of high-genistein soybean extract
(SOLGEN™, Tradichem SL, Madrid, Spain) and a proprietary pumpkin seed
extract (TradichemSL, Madrid, Spain), providing 22,5mg total of total
isoflavones (9 mggenistein plus genistin), 6.5mg pyrogallol and 8.75mg
enterodiol per tablet. The tablet also contained excipients/binders
including microcrystalline cellulose, silicon dioxide, magnesium
stearate, hydroxypropyl methylcellulose, stearic acid and titanium
dioxide. Tablets were manufactured by Eladiet S.A. Poli. Ind. Sud el
Papiol, Salvador Espriu, 32, 08754 El Papiol, Barcelona. SPAIN
Statistical analyses
Descriptive statistics, mean±standard deviation, were
used to summarize the data from the micturition diary. Paired
difference test (Wilcoxon test) was used to determine if there was a
significant improvement in the mean values of daily and nocturnal
frequency, urgency grade score, UUI, SUI and number of daily pantyliners
used between T0 and T2. Statistical significance was set at a P value
of 0.05.
Results
After eight weeks of treatment, the mean urgency
grade score was reduced by 24.7% (P<0.01) compared to baseline.
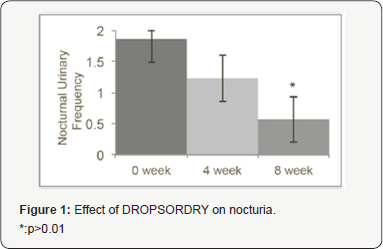
Nocturia was reduced by 69.35% (p<0.05, Figure 1) compared to baseline and the use of daily pantyliners was reduced by 66.25% (p<0.01, Figure 2)
compared to baseline. There was a trend in the reduction of SUI. In
addition, in the quality of life portion of the questionnaire, 96.2% of
subjects reported satisfaction with the treatment and 92.3% reported
improvement in quality of life. No side effects were reported.

Discussion
The present study investigated the effects of a
dietary supplement, DROPSORDRY™, on urinary incontinence in
perimenopausal women. There were a number of key finding. First,
statistically significant decreases were observed in two major symptoms
of UI-mean urgency grade, nocturia. In addition, there was a
statistically significant decrease in the use of daily panty liners,
indicating a reduction of involuntary urine loss. A reduction trend was
also observed in stress urinary incontinence. Finally, the majority of
subjects also reported improvement in quality of life and overall
satisfaction of the treatment; therefore, the present study's findings
indicate that DROPSORDRY™ can be an effective treatment to reduce
urinary incontinence symptoms in perimenopausal women within 8 weeks.
Changes in hormonal patterns during the transition
between perimenopause and menopausemay explain the increase in
prevalence of incontinence among women between the ages of 45 and 55
years [21].
Phytoestrogens have emerged as a natural alternative for treating
menopausal and perimenopausal symptoms. Unlike HRT, phytoestrogens do
not increase cancer or cardiovascular disease risk. In fact,
phytoestrogens have shown protective effects against cancer and
cardiovascular disease, as well as numerous other health benefits [18].
Soy is rich in phytoestrogens, particularly soy isoflavones, and has
been shown to exert positive estrogenic effects and reducing some
menopausal symptoms such as hot flashes [22] and loss of bone mineral density [23].
Genistein, which has structural similarities to 17β-estradiol (E2), has
been shown in animal models to reduce the expression of muscarinic
receptors M2 and M3 expression on the bladder wall. In addition,
genestein therapy also reduced morphological changes that contribute to
UI, such as increased collagen connective tissue and degenerative
changes to the bladder [12].
Circulating levels of androgens also gradually decrease with age in postmenopausal women [24].
Androgen receptors are also expressed in the pelvic floor and lower
urinary tract. Studies have also shown that androgens, like
testosterone, have a muscle-building effect on these muscles [25].
Since testosterone is normally converted to estradiol by the enzyme
aromatase, inhibition of aromatase may help maintain testosterone
levels. Pumpkin seed extracts and oil have been shown to inhibit
aromatase [26]. Which may explain why it has been used in folk medicine to treat kidney, bladder and prostate disorders [27] Pumpkin seed oil has also been shown to improve symptoms of overactive bladder [28].
Pumpkin seed extract in combination with soybean extracts have been
shown to have promising potential treat urinary tract complications
including SUI, overactive bladder, frequency and nocturia [29-32].
This study differs in that it focused solely on urinary incontinence in
perimenopausal women using a novel formula containing a soybean extract
containing a high level of genistein in combination with a proprietary
standardized pumpkin seed extract. Moreover, this is the first clinical
study conducted in Western women with occidental diet and non soy based
diet.
Conclusion
The results of this present study suggest that the
combination of phytoestrogens, particularly genistein, plus pyrogallol
from pumpkin seed, provide safe and effective estrogenic and androgenic
activity. This combination appears to help protect against both
biochemical and morphological changes that occur in menopausal
transition that increase the risk of urinary incontinence, resulting in
relief of UI symptoms and improved quality of life in perimenopausal
women.
For more open
access journals in JuniperPublishers please click on: https://juniperpublishers.com/
For more articles on Gynecology and Women’s
Health please click on: https://juniperpublishers.com/jgwh/


Comments
Post a Comment